
the epidemiology of the population it is to serve
its position in the health care system within its defined region and how external factors might influence its development
what would be a successful outcome for all stake holders (using SMART techniques)
the aspirations of the management and staff and career development patterns
the practicalities of service delivery and how any constraints might be addressed
We use specially developed software in all aspects of our design process, our Hiltron Planning System is built on current technologies but has its roots in systems developed and practically proven by our company in projects all over the World over the last 28 years.
Current systems use an Object Orientated approach using development languages including C# and Java. Standard design patterns are used allowing extension or access by other systems. In the past design teams have used pre-prepared departmental templates as a basis for architectural design, these templates are often “historical” and have failed to take account of rapidly changing medical procedures and technology. They often either include rooms which are no longer used and/or miss rooms which are required by modern practice including hospital IT, they also make assumptions about patient profiles which are not tested in the design process.
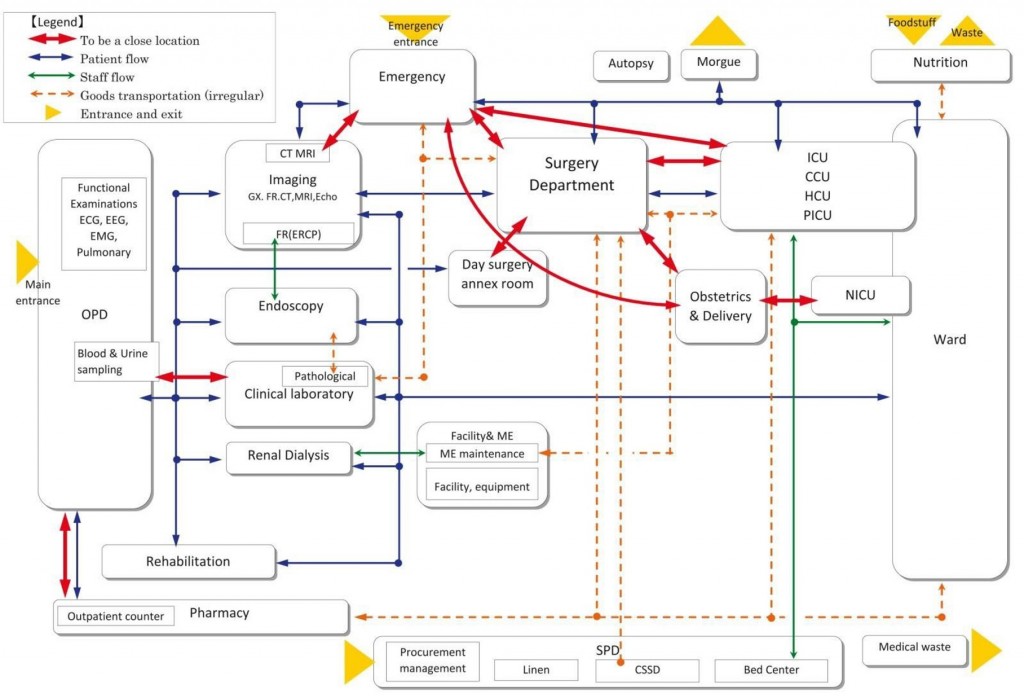
We consider each patient type shown to be required by epidemiology and practical local experience, how medical teams care for them and what facilities and services these teams require. We design for the individual needs of patients, staff, visitors etc.
Each hospital design is “tailor made” ensuring full support for modern requirements while saving space, energy and cost.
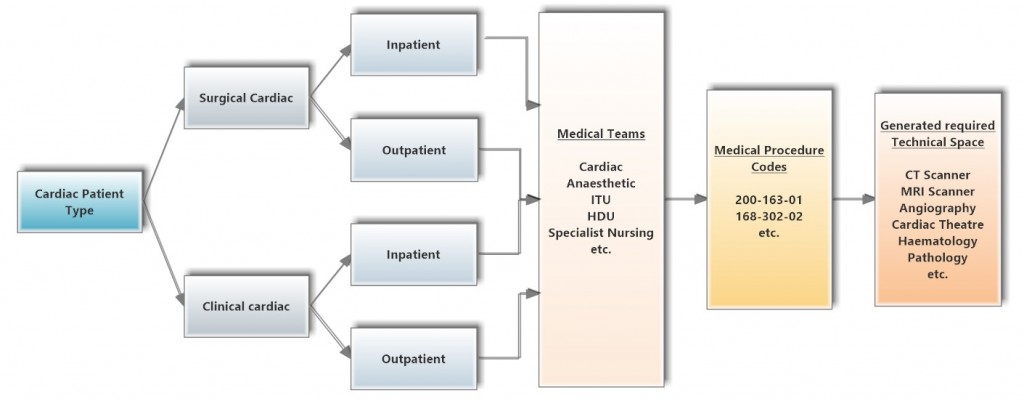
Our building block is the Patient, but in a majority of cases patients can be categorised by “type”, for example Surgical and Medical, and by Sub-type, for example Cardiac, Urology, Orthopaedics etc.
Modern medical practice will involve assigning a Medical Team to each patient type. We use the services needed by the Team (through a medical coding database) to test the requirement for technical rooms. Support Accommodation for Technical spaces AND Patient types is linked within the planning system as is equipment including services installation and specifications.
Modern hospitals are expensive to build, equip, staff and operate therefore design teams need to be able to consider all these inputs collectively and not just individually. Aided by our computer systems we are able to make use of a multi discipline approach to ensure best practices and value for money and use the data for future Operation and Maintenance.
Principles of design briefing
– Our design and briefing philosophy is based on an understanding of the care and treatment required by patients in the area which the project is to serve. This requires thorough analysis and documentation of local disease profiles (epidemiology) but also consideration of other local or national factors such as likely prevalence of accidental injury (is the project near a major road or airport?). It is also important to look at other local or national facilities and the general planning for optimisation of specialised services.
– Having established the type and likely numbers of various patient types we link these to the medical procedures which they are statistically likely to require and allow for a probability factor. For this process we use any current computer national medical coding, or recommend a suitable system such as that used in the USA and UK. These codes are extensive and detailed and can be used to imply the medical specialists required to carry them out, and also space planning and equipment and many other needs. Our system allows for development and extension of the coding to allow for local practices.
– Hence from the expected patient numbers we can develop an estimate of a wide range of other needs, such as medical staff numbers, space and equipment needs, catering, office space, laundry etc. etc.
Patterns & Data
– The major role of a consultancy such as Hiltron in the process described is to specify and provide template data for all of the processes required.
– We make extensive use of design patterns, but in contrast to previous systems ours are scheduled and drawn at a micro scale and allow for interchangeability, particularly allowing for local preferences and requirements. These design patterns link to the required medical codes.
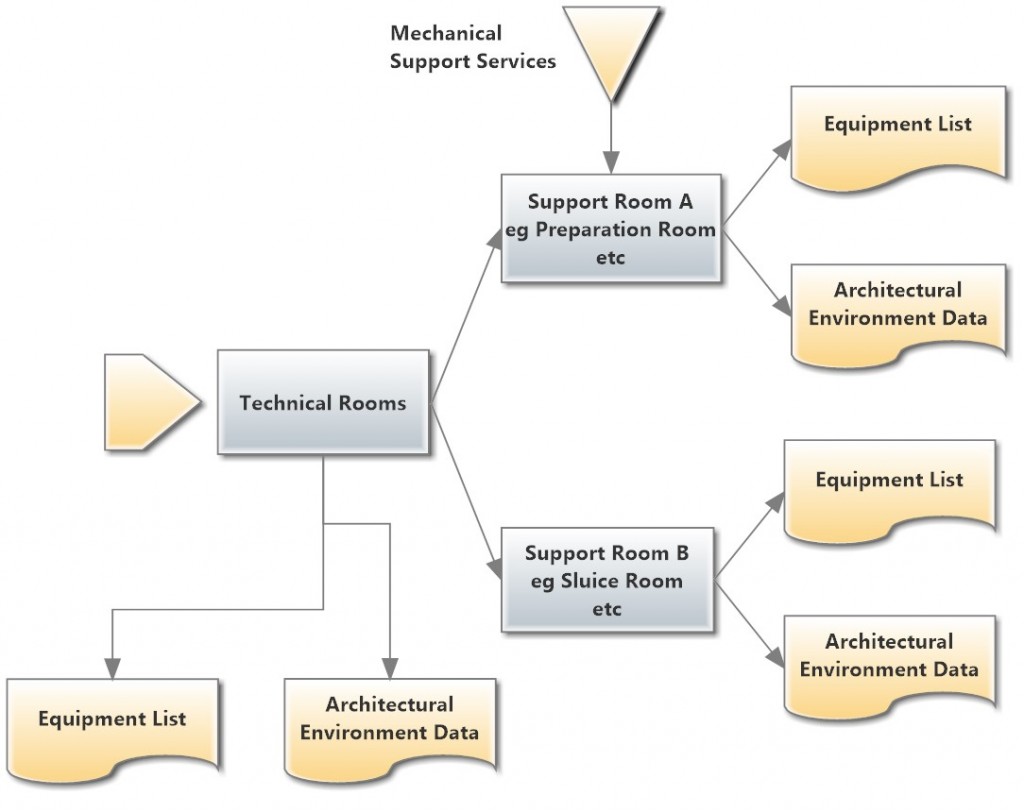
– Various academic works, for instance by Alexander et al, have identified that a pattern should enumerate in a pattern dictionary the problems addressed, how this solution addresses those problems and particular advantages and disadvantages. In our database we also include examples of associated parameters such as design area, service, energy and other requirements. The pattern should also indicate the need for other supporting patterns, for instance a 1 bed ward pattern should show not only the ward, en-suite etc. but the need for a sluice, treatment room. In our system these needs are further qualified by the quantum of time taken by the main pattern in the sub-pattern.
Medical Coding
– Medical procedure coding structures are used in various formats in different countries but one which enjoys considerable international support is SNOMED. This has been generally accepted in the USA and has suggested advantages as detailed in a presentation by Dr Roger A Cote
– Coding is used for a variety of statistical analysis and is also used in many countries as a basis for costing in private and insurance based medicine. It is usually structured to allow easy manipulation by computers.
– We have ensured that our system can accept a variety of coding structures, even those derived at a local level. However it is essential that the granularity of the codes is sufficient to enable unique identification of the resources required to support the indicated procedure. For instance it would not be sufficient to list a procedure requiring the use of an operating theatre without inferring the type of table, specialist medical staff, specialist equipment etc. required.
Scheduling of Resources
– Having identified the anticipated patient numbers and the probability of necessary treatment and procedures for each patient type it becomes possible to associate required support from staff, medical and other and other, and physical resources such as technical spaces and equipment.
– Each of the identified resources will in turn generate the need for other support. For instance the medical staff may well need an office and a range of other services such as catering, laundry and car parking.
– The essence of our briefing system is that example data allows semi-automatic completion of projected requirements once the initial patient numbers have been entered based on international experience. However it would be unduly optimistic to assume that there will be no variation in requirements at a local level and so each of the base parameters can be adjusted for individual projects.
Please click here to return to Services